MentalHealthCE Login


| Login | ||

Healthcare Training Institute - Quality Education since 1979
CE for Psychologist, Social Worker, Counselor, & MFT!!

Section 22
Clinically
Based Prediction Models in Assessing Dangerousness
Question 22 | Test | Table of Contents
The prediction of interpersonal violence demands the use of psychometrically
sound measurements and an understanding of such tools' limitations. Research in
clinical decision making (Benner, 1984; Harbison, 1991; Schon, 1983a) identifies
three major models for prediction: (a) the linear, rationalist model, (b) the
hypothetico-deductive model, and (c) the risk assessment model (Gottfredson &
Gottfredson, 1988). Depending on the goal of the assessment, the clinician may
use aspects of one or more of these models.
LINEAR
MODEL
Because prediction has such significant forensic implications,
clinicians may use a linear model, including a decision tree or critical pathway,
to guide them when making decisions that have legal ramifications. For example,
Gross, Southard, Lamb, and Weinberger (1987) propose seven steps to follow when
a client makes suggestive threats (see Figure 1.1).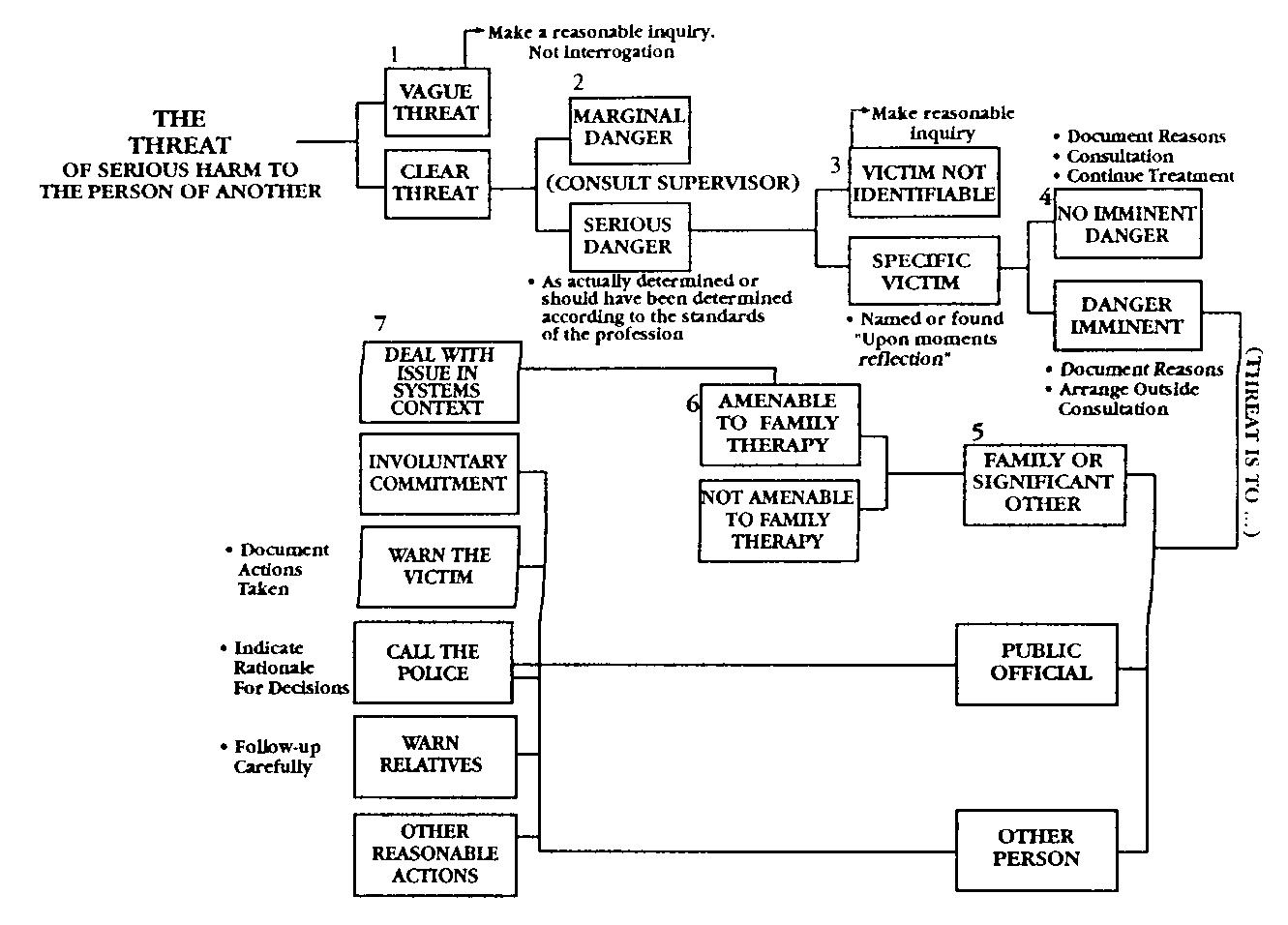
Thus, if there is a clear threat, Step 2 is to assess its lethality, as well as the likelihood of the person acting on the threat. As with suicidal thoughts, not all "threats" pose a true danger or can be enacted. The incarcerated client may verbalize specific threats of violence against someone outside of prison but have no means to carry through on the threats.
If there is evidence of danger, Step 3 is to identify a specific, intended victim. in family violence and family sexual assault cases, it is easy to identify intended victims. The violence is seldom random, even within homes in which multiple members reside. The clinician working with a client who is verbalizing concerns about physically and/or sexually assaulting a stranger may find it more difficult to identify a specific victim (by name). However, the clinician can ask the client to indicate the intended victim's gender and any specific victim characteristics.
If the client can name the intended victim or specifics about the type of victim who will be sought, the threat of harm is imminent (Step 4). At this point the clinician needs to consider his or her duty to warn the specified victim. For more detail the reader is referred to material on the Tarasoff decisions (Tarasoff v. Regents of the University of California, 1974, 1976).
The clinician also must take into account the client's relationship to the intended victim (Step 5). If the intended victim is a family member, rather than a political figure, the clinician may employ different preventive and treatment strategies.
Step 6 requires the clinician to decide whether a family therapy intervention would be suitable. For example, if the family violence is ongoing, family therapy may impose greater danger to the potential victim or victims.
Finally, Step 7 requires the clinician to consider whether civil commitment or involuntary hospitalization would provide the greatest good to the client and potential victim or victims. At the completion of Step 7, the clinician needs to follow up on the results of the decisions made and may need to recycle through the decision tree at a later date.
The strength of the linear model is that it
provides relatively clear direction for the clinician, as well as a "logical"
argument for the decision. Using the linear model, the clinician approaches problem
solving with some notion of probability. He or she weighs outcomes according to
objective standards or theory. The weakness of this model is also its objectivity;
contextually relevant information is given little consideration. In other words,
factors such as treatment outcomes, social support, and stabilization of stress
are not considered in making the prediction. The decision is driven by formula,
more than by the specifics of the actual situation.
- Campbell, Jacquelyn,
Assessing Dangerousness, Sage Publications: London, 1995.
Self-Injurious Behavior in Adolescents
- Whitlock J. (2010). Self-injurious behavior in adolescents. PLoS medicine, 7(5), e1000240. doi:10.1371/journal.pmed.1000240
Personal
Reflection Exercise #8
The preceding section contained information
about clinically based prediction models in assessing dangerousness. Write three
case study examples regarding how you might use the content of this section in
your practice.
Reviewed 2023
Update
Prediction model for suicide based on back propagation
neural network and multilayer perceptron
- Lyu, J., Shi, H., Zhang, J., & Norvilitis, J. (2022). Prediction model for suicide based on back propagation neural network and multilayer perceptron. Frontiers in neuroinformatics, 16, 961588. https://doi.org/10.3389/fninf.2022.961588
Peer-Reviewed Journal Article References:
Adrian, M., Berk, M. S., Korslund, K., Whitlock, K., McCauley, E., & Linehan, M. (2018). Parental validation and invalidation predict adolescent self-harm. Professional Psychology: Research and Practice, 49(4), 274–281.
Ammerman, B. A., Jacobucci, R., Turner, B. J., Dixon-Gordon, K. L., & McCloskey, M. S. (2020). Quantifying the importance of lifetime frequency versus number of methods in conceptualizing nonsuicidal self-injury severity. Psychology of Violence, 10(4), 442–451.
Nielsen, E., & Townsend, E. (2018). Public perceptions of self-harm—A test of an attribution model of public discrimination. Stigma and Health, 3(3), 204–218.
Siddaway, A. P., Wood, A. M., O'Carroll, R. E., & O'Connor, R. C. (2019). Characterizing self-injurious cognitions: Development and validation of the Suicide Attempt Beliefs Scale (SABS) and the Nonsuicidal Self-Injury Beliefs Scale (NSIBS). Psychological Assessment, 31(5), 592–608.
QUESTION
22
What is the strength in utilizing the linear model for assessing interpersonal
violence? To select and enter your answer go to Test.